FOR US HEALTHCARE PROFESSIONALS ONLY
Administration
This product requires a different preparation and administration than INVEGA SUSTENNA® and INVEGA TRINZA®. It is critical to prepare the medication following the instructions for use to ensure a complete injection of the full dose. Administering less than the full dose could negatively impact the patient’s outcome.
Important:
- INVEGA HAFYERA® requires longer and faster shaking than INVEGA SUSTENNA®
- INVEGA HAFYERA® should be administered by a healthcare professional as a single injection. DO NOT divide dose into multiple injections
- INVEGA HAFYERA® is intended for gluteal intramuscular use only. Inject slowly, deep into the muscle, taking care to avoid injection into a blood vessel
Instructions for Use Video
Instructions for Use
INVEGA HAFYERA® (paliperidone palmitate) is a highly concentrated product that requires specific shaking steps to ensure resuspension.
Proper dose preparation is required for complete resuspension of the medication and to reduce the risk of an incomplete injection that could lead to patients not experiencing a full therapeutic response.
INDICATION
INVEGA HAFYERA®, an every-six-month injection, is an atypical antipsychotic indicated for the treatment of schizophrenia in adults after they have been adequately treated with:
- A once-a-month paliperidone palmitate extended release injectable suspension (e.g., INVEGA SUSTENNA®) for at least four months or
- An every-three-month paliperidone palmitate extended release injectable suspension (e.g., INVEGA TRINZA®) for at least one three-month cycle.
INVEGA TRINZA® is an atypical antipsychotic indicated for the treatment of schizophrenia in patients after they have been adequately treated with INVEGA SUSTENNA® for at least four months.
INVEGA SUSTENNA® is an atypical antipsychotic indicated for the treatment of schizophrenia in adults.
IMPORTANT SAFETY INFORMATION.
Warning: increased mortality in elderly patients with dementia-related psychosis. See full prescribing information for complete boxed warning. Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. INVEGA HAFYERA®, INVEGA TRINZA® and INVEGA SUSTENNA® are not approved for use in patients with dementia-related psychosis.
Watch this video until the end and follow the steps to ensure proper resuspension and a complete injection. It is critical to prepare the medication correctly to ensure patients get the full dose. Administering less than the full dose could negatively impact the patient's outcome.
- INVEGA HAFYERA® (paliperidone palmitate) requires longer and faster shaking than INVEGA SUSTENNA® (paliperidone palmitate) and INVEGA TRINZA® (paliperidone palmitate).
- INVEGA HAFYERA® should be administered by a healthcare professional as a single injection.
- Do not divide the dose into multiple injections.
- INVEGA HAFYERA® is intended for gluteal intramuscular injection only. Do not inject by any other route.
- INVEGA HAFYERA® is injected to the upper outer quadrant of the gluteal muscle. Therefore, there is no need for your patient to fully disrobe.
- Inject slowly, deep into the muscle, taking care to avoid injection into a blood vessel.
- Injections should be alternated between the two gluteal muscles.
Before we get started, here's what the syringe looks like. This is the syringe tip cap, the Luer connection, the finger flange, and the plunger. For this injection, use only the provided 20G x 1.5-inch thin wall safety needle included in this kit. This is the yellow hub. This is the needle sheath. Now, let's get started.
Step one: Prepare for the injection. Pay close attention to the following steps. To ensure complete resuspension, shake the syringe with the tip cap pointing up. It's important that you shake with a short, very fast, up-and-down motion with a loose wrist for at least 15 seconds. 13, 14, 15. Done. Rest briefly. Now, shake again for an additional 15 seconds. 28, 29, 30. Done. Proceed to the next step immediately after shaking. Now, check the suspension for solid product. It should look uniform, thick, and milky white. It is normal to see air bubbles.
If it is not mixed well, you will see solid product on the sides and top of the syringe, or the mix may look uneven or the liquid may look thin. Stop: Product may clog.
Repeat shaking the syringe very fast with the syringe tip cap pointing up for at least 15 seconds. Rest briefly, then shake again for 15 seconds. You now have five minutes to inject the medication.
If more than five minutes pass before the injection, shake very fast for at least 30 seconds with the syringe tip cap pointing up to resuspend the medication. Open the needle pouch and place pouch with the needle inside on a clean surface. Hold the syringe with syringe tip cap pointing up, twist and pull off the cap. Attach the safety needle to the syringe using a gentle twisting motion to avoid needle hub cracks or damage. Always check for signs of damage or leakage prior to administration. Only use the needle included in this kit. Hold the syringe upright, and gently pull back the plunger to clear the syringe tip of any solid product. This will make pressing the plunger easier during the injection. To remove any air bubbles, press the plunger carefully until a drop of liquid comes out of the needle tip.
Step two: Slowly inject entire content and confirm. Select and clean a gluteal injection site. Do not administer by any other route. Because INVEGA HAFYERA® is injected into the upper outer quadrant of the gluteal muscle, there is no need for your patient to fully disrobe. Wipe the injection site with an alcohol swab and allow to dry. Do not touch, fan, or blow on the injection site after you have cleaned it. Finally, remove the needle sheath. Pull the needle sheath away from the needle in a straight motion. Do not twist the sheath, as this may loosen the needle from the syringe. Slowly inject and confirm that the entire content of the syringe has been injected by using slow, firm consistent pressure to press the plunger completely. This should take approximately 30 seconds. Continue pressing the plunger if you feel resistance. This is normal. While the needle is in the muscle, confirm that the entire content of the syringe has been injected. Remove the needle from the muscle.
Step three: After the injection. After the injection is complete, use your thumb or a flat surface to secure the needle in the safety device. The needle is secure when you hear a click sound. Dispose of the used syringe in an approved sharps container and check the injection site. There may be a small amount of blood or liquid at the injection site. Hold pressure on the skin with a cotton ball or gauze pad until any bleeding stops. Do not rub the injection site. If needed, cover the injection site with a bandage. Your injection is now complete. For additional information, please review the included printed instructions for use.
As a reminder
INVEGA HAFYERA® requires longer and faster shaking than INVEGA SUSTENNA® and INVEGA TRINZA®. It's important that you shake the syringe with the tip cap pointing up with a short, very fast, up-and-down motion with a loose wrist for at least 15 seconds. Done. Rest briefly, then shake again for an additional 15 seconds.
INVEGA HAFYERA® is to be injected into the upper outer quadrant of the gluteal muscle.
Thank you for watching this video. Please continue watching to view important safety information, including boxed warning, for INVEGA HAFYERA®.
INDICATION
INVEGA HAFYERA®, an every-six-month injection, is an atypical antipsychotic indicated for the treatment of schizophrenia in adults after they have been adequately treated with:
- A once-a-month paliperidone palmitate extended release injectable suspension (e.g., INVEGA SUSTENNA®) for at least four months or
- An every-three-month paliperidone palmitate extended release injectable suspension (e.g., INVEGA TRINZA®) for at least one three-month cycle.
INVEGA TRINZA® is an atypical antipsychotic indicated for the treatment of schizophrenia in patients after they have been adequately treated with INVEGA SUSTENNA® for at least four months.
INVEGA SUSTENNA® is an atypical antipsychotic indicated for the treatment of schizophrenia in adults.
IMPORTANT SAFETY INFORMATION
WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS.
See full prescribing information for complete Boxed Warning.
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. INVEGA HAFYERA®, INVEGA TRINZA® and INVEGA SUSTENNA® are not approved for use in patients with dementia-related psychosis.
Contraindications. INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® are contraindicated in patients with a known hypersensitivity to either paliperidone, risperidone, or to any excipients of their formulation.
Cerebrovascular adverse reactions. Cerebrovascular adverse reactions, for example, stroke, transient ischemic attacks, including fatalities, were reported at a higher incidence in elderly patients with dementia-related psychosis taking risperidone, aripiprazole, and olanzapine compared to placebo. No studies have been conducted with oral paliperidone, INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA® in elderly patients with dementia. These medications are not approved for the treatment of patients with dementia-related psychosis.
Neuroleptic malignant syndrome (NMS). NMS, a potentially fatal symptom complex, has been reported in association with antipsychotic drugs, including paliperidone. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status, including delirium and autonomic instability (irregular pulse of blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine, phosphokinase, myoglobinuria, rhabdomyolysis, and acute renal failure. If NMS is suspected, immediately discontinue INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA®, and provide symptomatic treatment and monitoring.
QT prolongation. Paliperidone causes a modest increase in the corrected QT (QTc) interval. Avoid the use of drugs that also increase QTc interval and in patients with risk factors for prolonged QTc interval.
Paliperidone should also be avoided in patients with congenital long QT syndrome and in patients with a history of cardiac arrhythmias. Certain circumstances may increase the risk of the occurrence of torsades de pointes and/or sudden death in association with the use of drugs that prolong the QTc interval.
Tardive dyskinesia (TD). TD, a syndrome consisting of potentially irreversible, involuntary, dyskinetic movements may develop in patients treated with antipsychotic drugs. Although the prevalence of the syndrome appears to be highest among the elderly, especially elderly women, it is impossible to predict which patients will develop the syndrome. Whether antipsychotic drug products differ in their potential to cause tardive dyskinesia is unknown.
The risk of developing TD, and the likelihood that it will become irreversible, appear to increase with the duration of treatment and the cumulative dose. The syndrome can develop after relatively brief treatment periods, even at low doses. It may also occur after discontinuation. TD may remit partially or completely if antipsychotic treatment is discontinued. Antipsychotic treatment itself, however, may suppress or partially suppress the signs and symptoms of the syndrome possibly masking the underlying process. The effect that symptomatic suppression has upon the long-term course of the syndrome is unknown.
If signs and symptoms of TD appear in a patient on INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA®, drug discontinuation should be considered. However, some patients may require treatment with INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA® despite the presence of the syndrome. In patients who do require chronic treatment, use the lowest dose and the shortest duration of treatment, producing a satisfactory clinical response. Periodically reassess the need for continued treatment.
Metabolic changes. Atypical antipsychotic drugs have been associated with metabolic changes that may increase cardiovascular/cerebrovascular risk. These metabolic changes include hyperglycemia, dyslipidemia, and body weight gain. While all of the drugs in the class have been shown to produce some metabolic changes, each drug has its own specific risk profile.
Hyperglycemia and diabetes mellitus: Hyperglycemia and diabetes mellitus, in some cases extreme and associated with ketoacidosis, hyperosmolar coma or death have been reported in patients treated with all atypical antipsychotics (APS). Patients starting treatment with APS who have or are at risk for diabetes mellitus should undergo fasting blood glucose testing at the beginning of and during treatment. Patients who develop symptoms of hyperglycemia during treatment should also undergo fasting blood glucose testing. All patients treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia. Some patients require continuation of antidiabetic treatment despite discontinuation of the suspect drug.
Dyslipidemia. Undesirable alterations have been observed in patients treated with atypical antipsychotics.
Weight gain. Weight gain has been observed with atypical antipsychotic use. Clinical monitoring of weight is recommended.
Orthostatic hypotension and syncope. INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® may induce orthostatic hypotension in some patients due to its alpha-adrenergic blocking activity. INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® should be used with caution in patients with known cardiovascular disease, cerebrovascular disease or conditions that would predispose patients to hypotension (for example, dehydration, hypovolemia, treatment with antihypertensive medications). Monitoring should be considered in patients for whom this may be of concern.
Falls. Somnolence, postural hypotension, motor and sensory instability have been reported with the use of antipsychotics, including INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA®, which may lead to falls and consequently fractures or other fall-related injuries. For patients, particularly the elderly with diseases, conditions, or medications that could exacerbate these effects, assess the risk of falls when initiating antipsychotic treatment and recurrently for patients on long-term antipsychotic therapy.
Leukopenia, neutropenia, and agranulocytosis have been reported with antipsychotics, including INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA®. In patients with a history of clinically significant low white blood cell count (WBC)/absolute neutrophil count (ANC) or drug-induced leukopenia/neutropenia, perform a complete blood count frequently during the first few months of therapy. Consider discontinuing INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® at the first sign of a clinically significant decline in WBC in the absence of other causative factors. Monitor patients with clinically significant neutropenia for fever or other symptoms or signs of infection, and treat promptly if such symptoms or signs occur. Discontinue INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® in patients with severe neutropenia (absolute neutrophil count less than 1000/mm3) and follow their WBC until recovery.
Hyperprolactinemia. As with other drugs that antagonize dopamine D2 receptors, INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® elevate prolactin levels, and the elevation persists during chronic administration. Paliperidone has a prolactin-elevating effect similar to risperidone, which is associated with higher levels of prolactin elevation than other antipsychotic agents.
Potential for cognitive and motor impairment. Somnolence, sedation, and dizziness were reported as adverse reactions in subjects treated with INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA®. INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® have the potential to impair judgment, thinking, or motor skills. Patients should be cautioned about performing activities that require mental alertness such as operating hazardous machinery, including motor vehicles, until they are reasonably certain that INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® do not adversely affect them.
Seizures. INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® should be used cautiously in patients with a history of seizures or with conditions that potentially lower seizure threshold. Conditions that lower seizure threshold may be more prevalent in patients 65 years or older.
Administration, for intramuscular injection only by a healthcare professional using only the needles provided in the INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA® kits. Care should be taken to avoid inadvertent injection into a blood vessel.
Drug interactions. Strong CYP3A4/P-glycoprotein (P-gp) inducers. Avoid using a strong inducer of CYP3A4 and/or P-gp (for example, carbamazepine, rifampin, St. John's Wort) during a dosing interval for INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA®. If administering a strong inducer is necessary, consider managing the patient using paliperidone extended-release tablets.
Pregnancy/Nursing. INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® may cause extrapyramidal and/or withdrawal symptoms in neonates with third trimester exposure. Advise patients to notify their healthcare professional if they become pregnant or intend to become pregnant during treatment with INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA®. Patients should be advised that there is a pregnancy registry that monitors outcomes in women exposed to INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA® during pregnancy. INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA® can pass into human breast milk. The benefits of breastfeeding should be considered along with the mother's clinical need for INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA®, and any potential adverse effect on the breastfed infant from INVEGA HAFYERA®, INVEGA TRINZA®, or INVEGA SUSTENNA®, or the mother's underlying condition.
Commonly observed adverse reactions for INVEGA HAFYERA®. The most common adverse reactions (incidence at least 5% in the double-blind phase) in the INVEGA HAFYERA® year clinical trial were upper respiratory tract infection, injection site reaction, weight increased, headache, and parkinsonism.
Commonly observed adverse reactions for INVEGA TRINZA®. The most common adverse reactions (incidence greater than or equal to 5% and occurring at least twice as often as placebo) were injection site reaction, weight increased, headache, upper respiratory tract infection, akathisia, and parkinsonism.
Commonly observed adverse reactions for INVEGA SUSTENNA®. The most common adverse reactions in clinical trials in patients with schizophrenia (incidence greater than or equal to 5% and occurring at least twice as often as placebo) were injection site reactions, somnolence, sedation, dizziness, akathisia, and extrapyramidal disorder.
Please read the full Prescribing Information, including Boxed WARNING, for INVEGA HAFYERA®, INVEGA TRINZA®, and INVEGA SUSTENNA®.
Preparing and injecting INVEGA HAFYERA®1
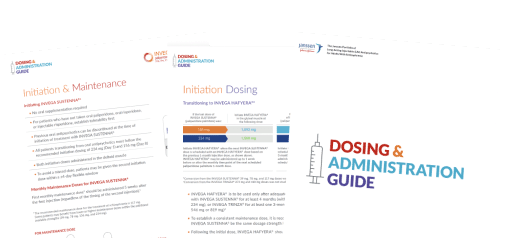
STEP 1
Holding the syringe with the tip cap pointing up, shake the syringe with a loose wrist, using a very fast up-and-down motion, for at least 15 seconds.
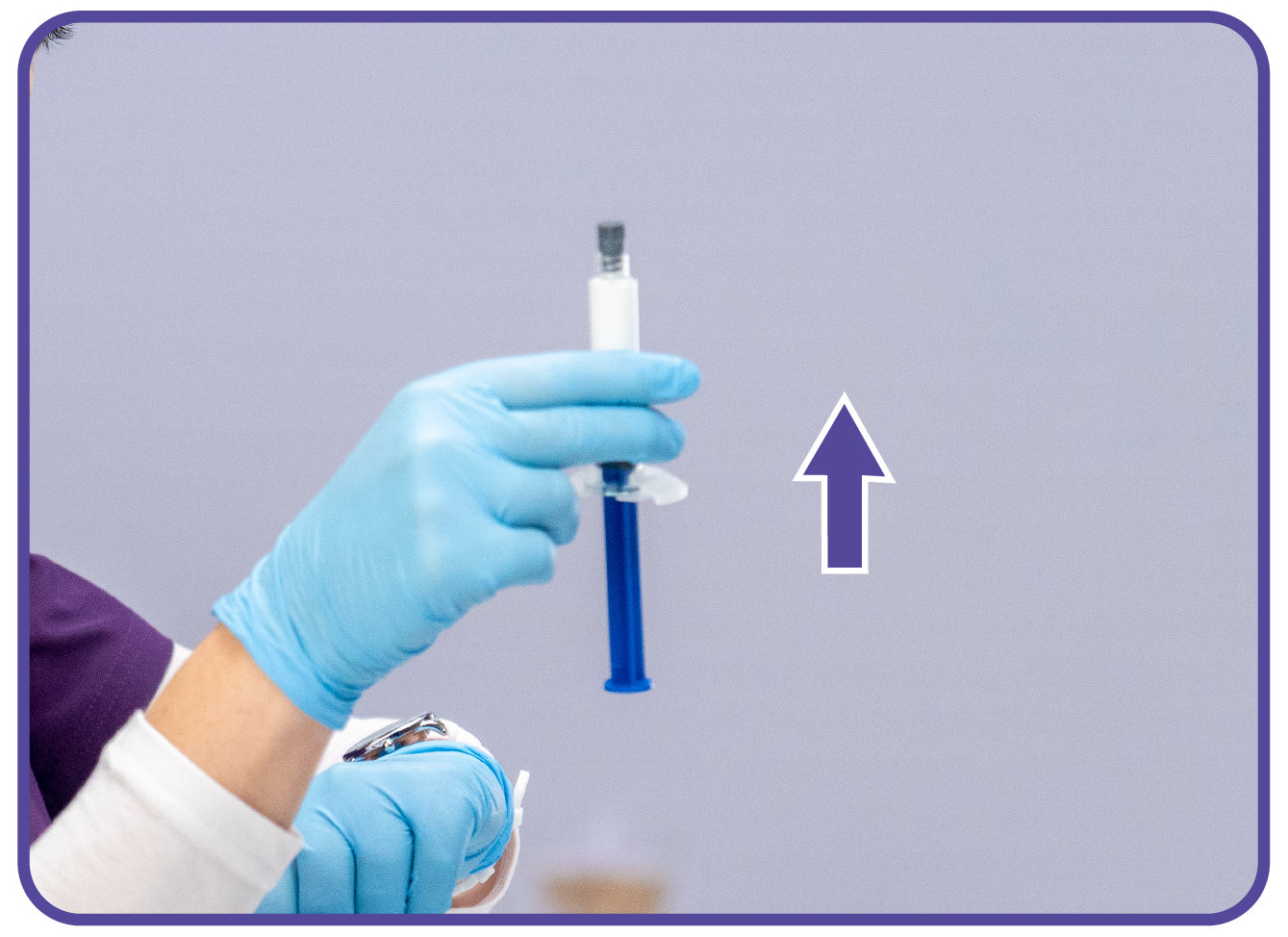
STEP 2
Rest briefly, then shake again in the same way, using a very fast up-and-down motion with a loose wrist for an additional 15 seconds.

STEP 3
Check suspension to ensure it is uniform, thick and milky white. It is normal to see air bubbles.
If it is solid on the sides and top of syringe, it is an uneven mix, or it is a thin liquid, STOP. The product may clog.
Shake syringe with the syringe tip cap pointing up VERY FAST for at least 15 seconds, rest, then shake again for 15 seconds.

STEP 4
Proceed immediately to inject INVEGA HAFYERA®.
- INVEGA HAFYERA® must be injected into the gluteal muscle only, using the 1½-inch, 20-gauge needle provided (regardless of patient's weight)
- Do not administer by any other route
- INVEGA HAFYERA® is injected into the upper-outer quadrant of the gluteal muscle, so there is no need for your patient to fully disrobe
- Use slow, firm, consistent pressure to press the plunger completely. This should take approximately 30 seconds. Continue to press the plunger if you feel resistance. This is normal. While the needle is in the muscle, confirm that the entire content of the syringe has been injected
- If more than 5 minutes pass before the injection is administered, shake the syringe again very fast with the tip pointing up for at least 30 seconds to resuspend the medication
- Alternate injections between the left and right gluteal muscles
Reference: 1. INVEGA HAFYERA® [Prescribing Information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.